A tissue flap procedure (also known as autologous tissue reconstruction or tissue-based reconstruction) is one way to rebuild the shape of your breast after surgery to remove the cancer. As with any surgery, you should learn as much as possible about the benefits and risks, and discuss them with your doctor, before having the surgery.
On this pageThese procedures use tissue from other parts of your body, such as your tummy, back, thighs, or buttocks to rebuild the breast shape. Tissue flaps look and feel more natural and act more like natural breast tissue than breast implants. Unlike implants, tissue flaps will change like any other tissue in your body. For instance, they may get bigger or smaller as you gain or lose weight. And while breast implants sometimes need to be replaced (if the implant ruptures, for example), this is not a concern with tissue flaps. Tissue flaps are often used by themselves to reconstruct the breast, but some tissue flap procedures can be used with a breast implant if more volume is needed.
Tissue flap procedures can also have some downsides that need to be considered:
There are many different types of flap procedures. They are often named by the muscle or artery that is being used and they mainly fall in two groups:
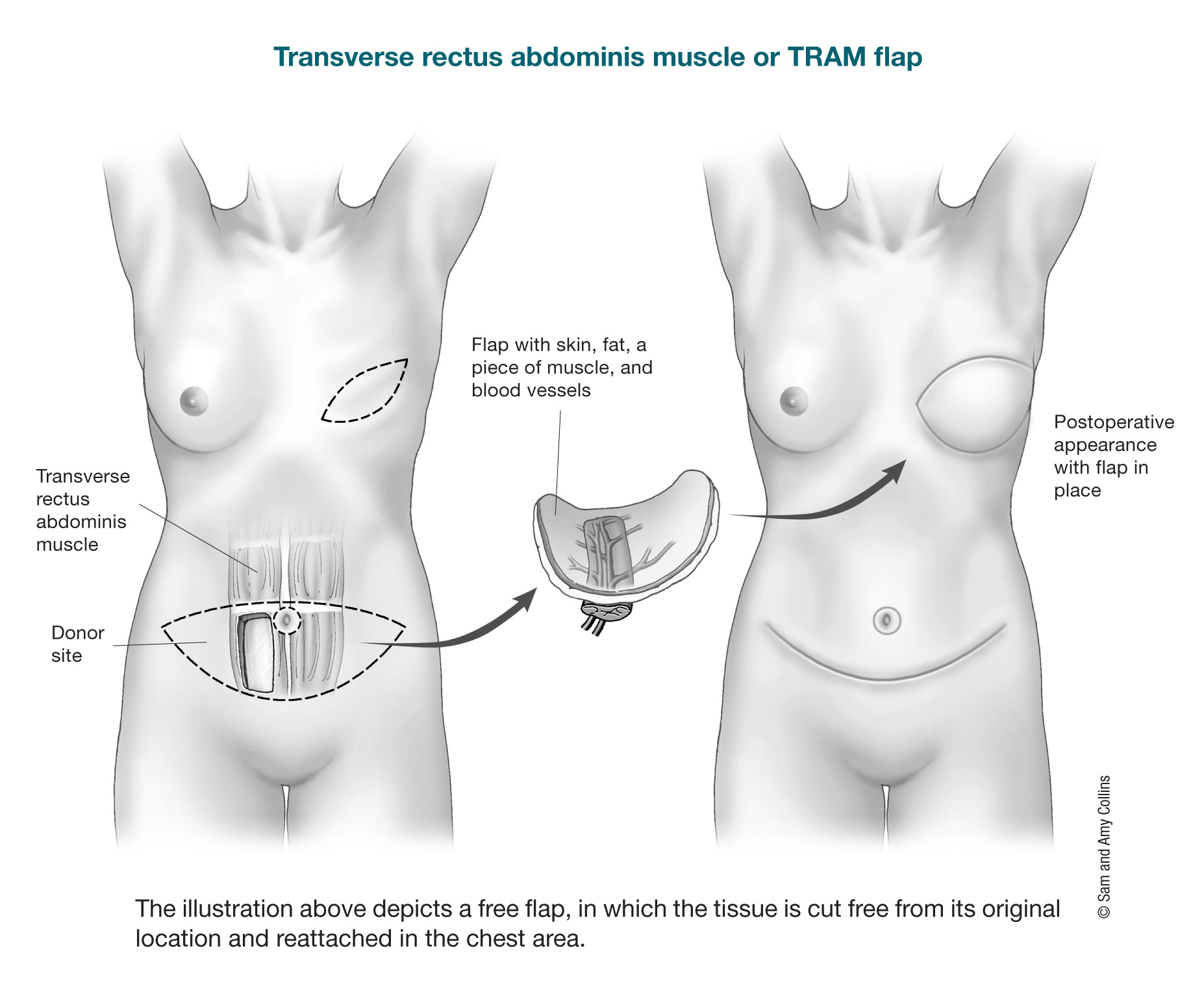
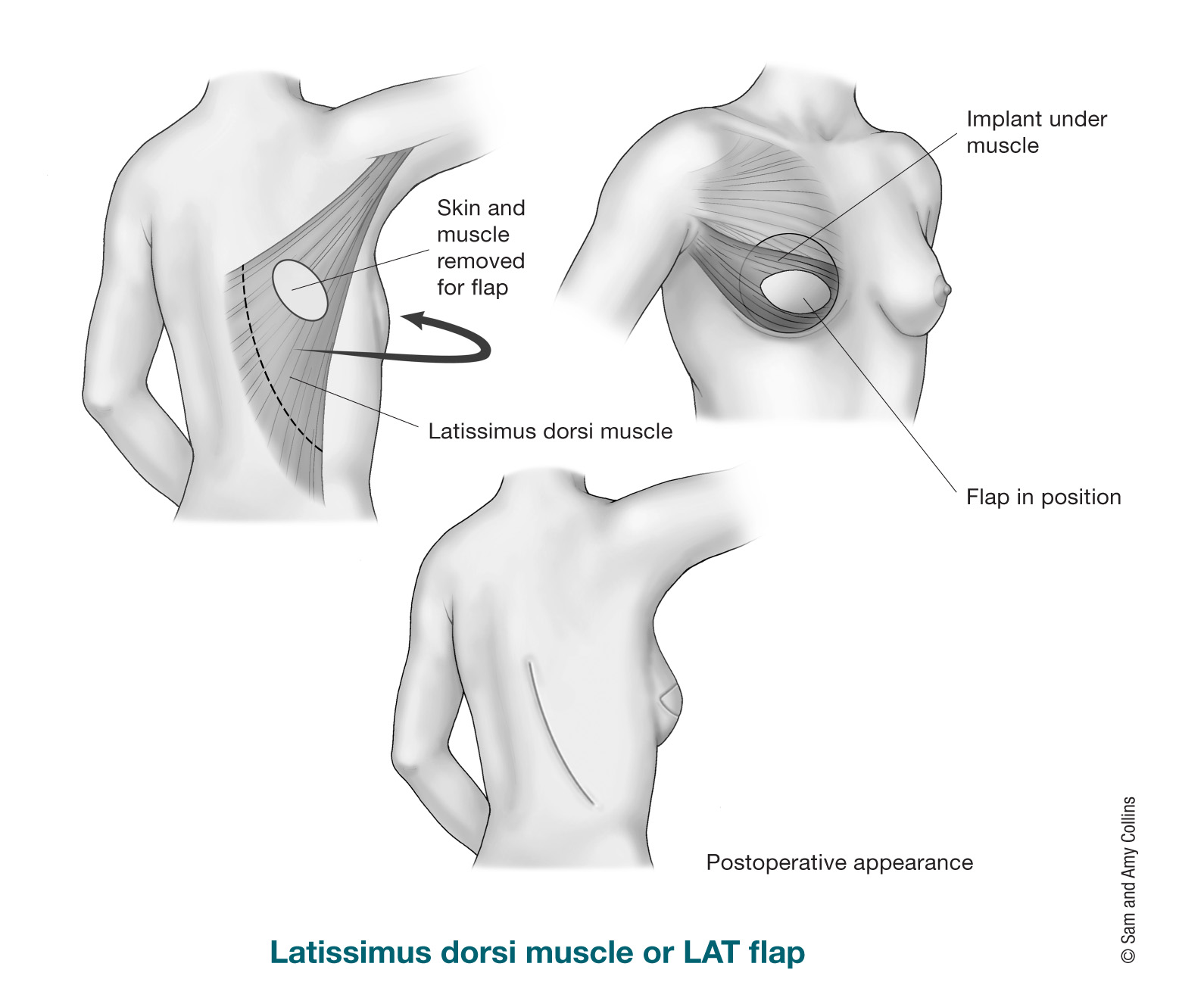
Pedicle flaps: A pedicle flap moves tissue from its site to the breast or chest wall while it is still attached to its original blood supply. The most common pedicle flap used for breast reconstruction is the latissimus dorsi (LD) flap, where tissue from the back (skin, fat, and muscle) is used to make a new breast. Tissue from the abdominal wall (tummy) can also be used as a pedicle flap (transverse rectus abdominis muscle or TRAM flap). But this has been largely replaced by its free flap version, where the muscle can be totally or partially saved.
Free flaps: A free flap moves tissue, fat, skin, and some or none of the muscle from one area of the body to make a new breast. This tissue is completely removed from the body and moved up to the chest. The blood vessels (arteries and veins) must then be reconnected to the chest wall vessels for the tissue to survive. This requires the use of a microscope (microsurgery) to connect the tiny vessels, and the surgery takes longer than a pedicle flap. Most of the time, free flaps don't need to take the muscle from the donor site, so there is less risk of losing muscle strength, and the donor site often looks better than if the muscle had been removed. The main risk is that sometimes the blood vessels get clogged and the flap doesn’t work because of poor or no blood supply. The abdominal wall (tummy) is the most popular and common donor site for free flap breast reconstruction. Other possible donor site areas for breast free flap reconstruction are the thighs, buttocks, and lower back.
During a mastectomy, nerves are cut causing a loss of sensation (feeling) on that side. The skin on the chest wall can feel numb (no feeling) or be more sensitive. The feeling might return after a few months or years or not at all. Finding ways to restore the feeling in the reconstructed breast has become a goal of tissue (flap) breast reconstruction. It is often possible to keep a sensory nerve (a nerve that controls feeling) within the flap. On the chest wall, a nerve in between the ribs is isolated and then reconnected with the nerve of the flap. This connection helps stimulate the tissue flap to regain feeling. There are studies that show improvement of sensation using this technique.
An abdominal wall flap procedure uses tissues from the tummy. Most times the tummy provides enough tissue for breast reconstruction, so no breast implants are needed. The tummy flap names are based on how the tissue is transferred and if the abdominal wall muscle is used or not. The donor site of the abdominal wall flap may look like a “tummy tuck,” but it can also reduce the strength in your belly muscles and cause bulging depending on what technique was used. Tummy flaps may not be possible in women who are very thin or who have had a tummy tuck before.
There are different types of abdominal wall (tummy) flaps:
A free muscle-sparing TRAM (MS-TRAM) flap is like a free TRAM flap except only part of the muscle from the same part of the lower abdomen, is completely removed and moved up to the chest. The blood vessels (arteries and veins) must then be reattached with microsurgery. Here the plastic surgeon saves most of the abdominal wall muscles; only a small piece of muscle is taken with the flap. There is less risk of abdominal wall bulging and losing abdominal muscle strength, and the donor site (abdomen) often looks better.
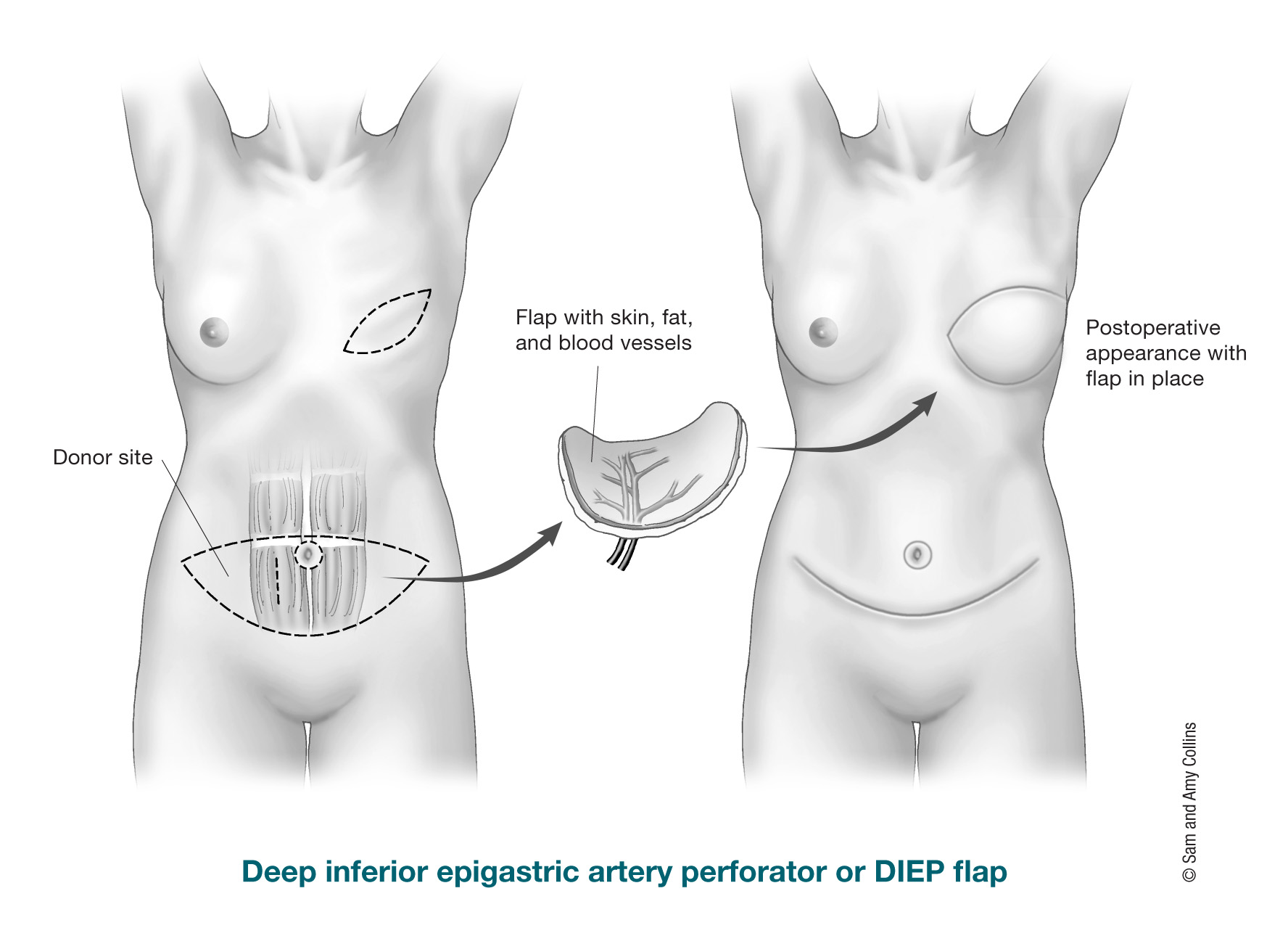
The DIEP (deep inferior epigastric perforator) free flap uses fat and skin from the same area as the TRAM flap to form the breast shape. The difference compared to a free TRAM flap is that no muscle is taken from the abdominal wall. The tissue is completely cut free from the tummy and then moved to the chest. As in the free TRAM flap surgery, a microscope is needed to connect the tiny blood vessels. There’s much less risk of a bulge because no muscle is taken. The free MS-TRAM flap and DIEP free flap are very similar to each other; in one (MS-TRAM flap) you just take a small piece of muscle, and in the other one (DIEP flap) no muscle.
Another possible abdominal wall (tummy) flap is the SIEA (superficial inferior epigastric artery) free flap. Basically, it uses the same tissues as the TRAM and DIEP flaps, but different blood vessels. The blood vessels used for the SIEA flap are more superficial (shallow) and not every person has them. Very few people are candidates for a SIEA flap.
The latissimus dorsi flap is a pedicle flap used for breast reconstruction. Since there is usually not as much tissue there as from an abdominal wall (tummy) donor site, this type of flap is often used with a breast implant to add volume (size) to breast reconstruction. For this procedure, the surgeon tunnels muscle, fat, skin, and blood vessels from your upper back, under the skin to the front of the chest. This type of reconstruction can sometimes be used without an implant depending on the amount of tissue and the desired breast size. Even though one muscle from the back is taken with the flap, rarely do women have weakness in their back, shoulder, or arm after this surgery.
There are also pedicle back flaps that do not take any muscle. The thoracodorsal artery perforator (TDAP) flap takes skin and fat from the upper back, but does not take any muscle. It is usually used for reconstruction after lumpectomy or partial mastectomy when needed.
A newer type of procedure, called a lumbar artery perforator (LAP) free flap, might be an option if there is not enough abdominal wall (tummy) tissue to use as a donor site . The skin, fat, and blood vessels are removed from the lower back area (also sometimes called “love handles”) and moved to the chest and the blood vessels are reconnected. No muscle is removed. The LAP free flap can only be done on one side at a time (one breast at a time), has an extra step to reconnect the blood vessels, and it is offered only at a few hospitals in the US.
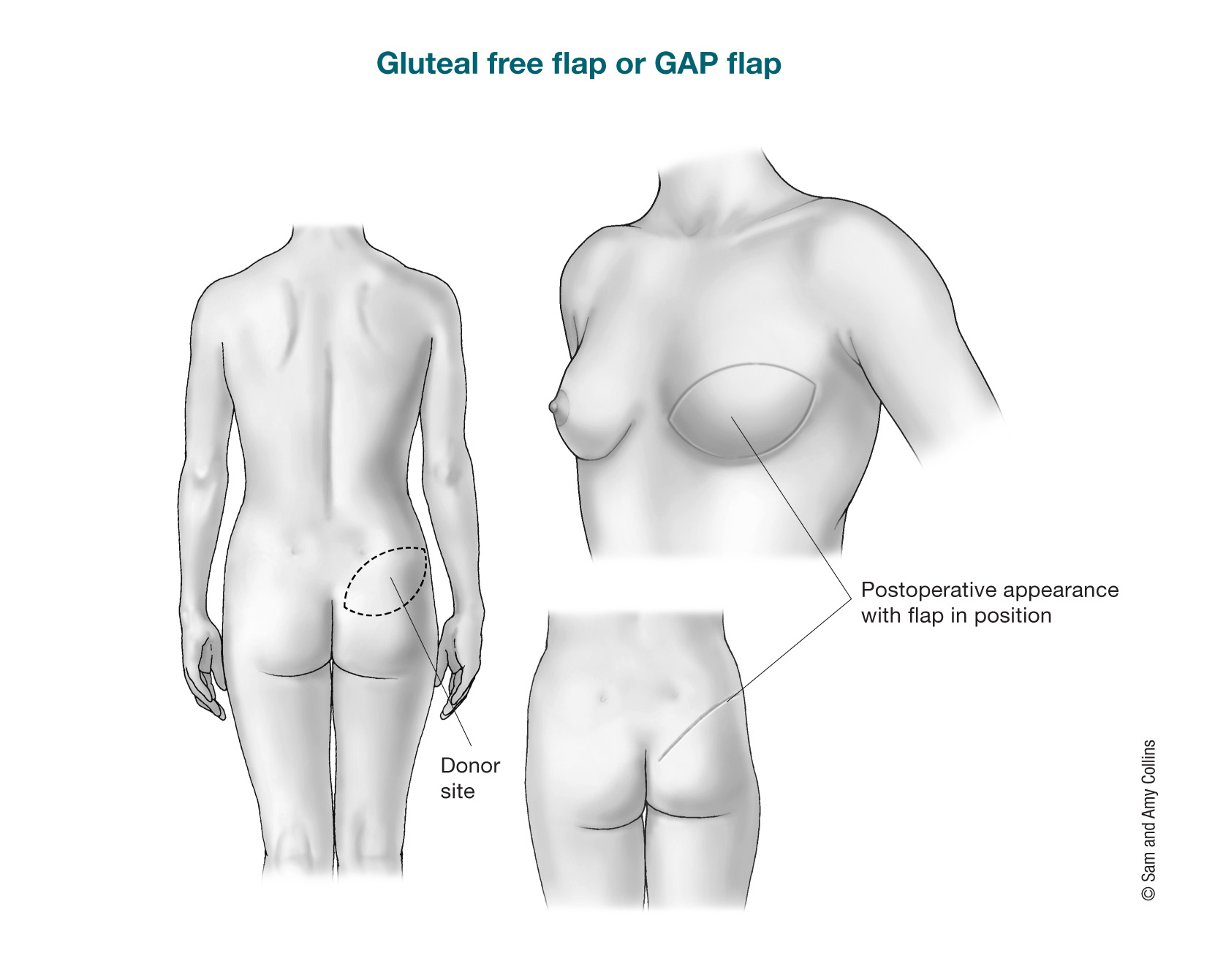
The gluteal free flap or gluteal artery perforator (GAP) flap uses tissue from the buttocks (bottom) to create the breast shape. The gluteal free flap might be an option for women who cannot or do not wish to use the tummy site because they are thin, have previous incisions, have had a previous tummy tuck, or for other reasons, but it’s not offered at all surgical centers. The skin, fat, and blood vessels are cut out of the buttocks and then moved to the chest. No muscle is removed. The blood vessels will also be reattached. You might see this type of flap called a superior gluteal artery perforator (SGAP) flap if the artery in the upper buttocks is used. The IGAP flap (inferior gluteal artery perforator flap) is a similar surgery except the artery in the bottom part of the buttocks is used. The major drawback of this flap is the possible change in the buttock contour, such as skin dimpling. For this reason, it has not become very popular.
If tissue from the abdominal wall (tummy) cannot be used, the tissues in the thighs are often looked at for breast reconstruction.
Depending on a women's body build and preferences, there are good free flap options from tissues of the inner and outer thighs. All the options require the use of microsurgery and reconnection of the blood vessels in the chest. Most of the time, the thighs only provide enough tissue to make a small or medium-sized breast. In some cases, two flaps, each one from a different thigh, can be used to reconstruct one breast.
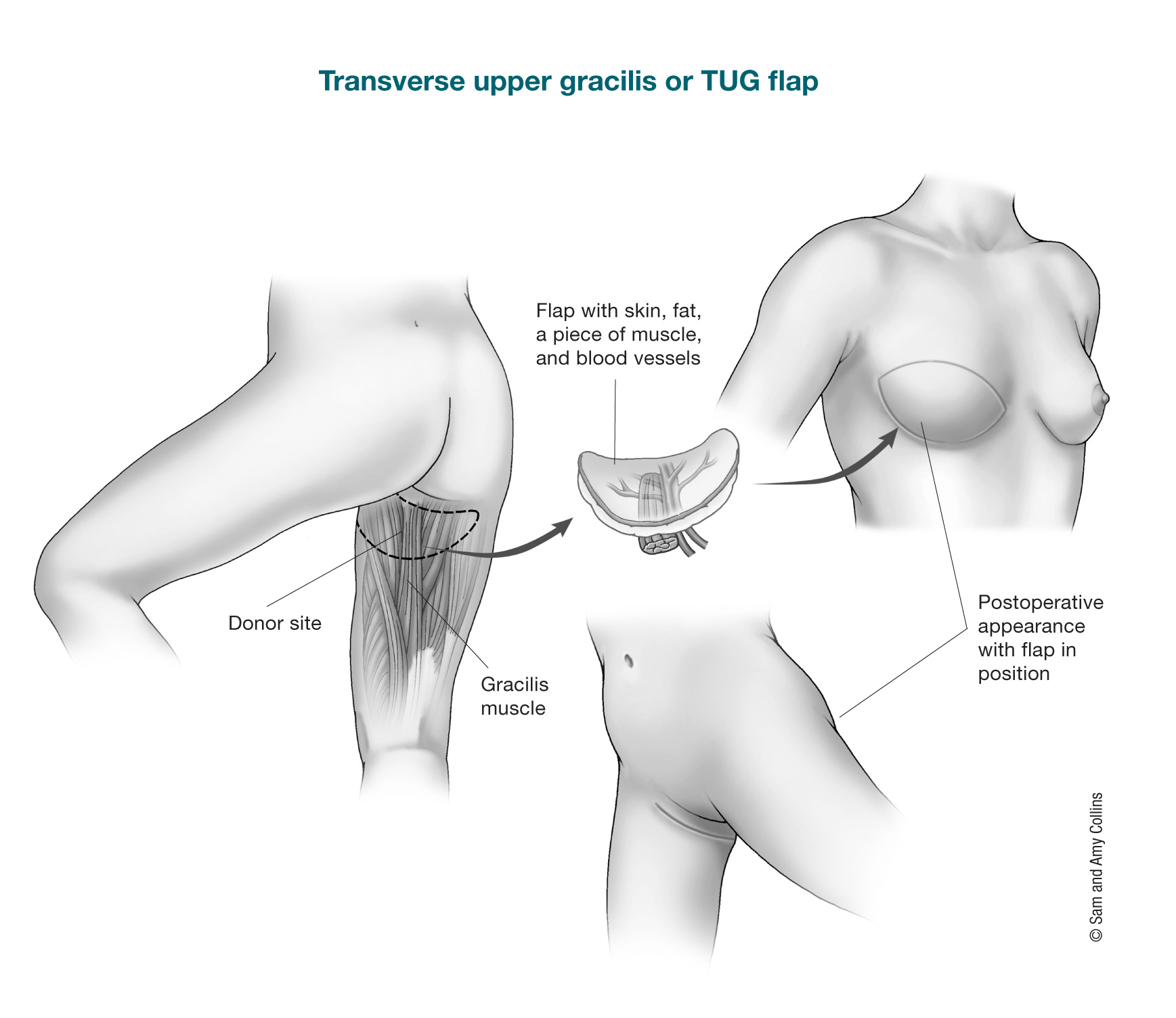
Inner thigh: The main options for free flaps from the inner thighs are.
Outer thigh: Another option for women who might have more fatty tissue on the outer part of their thighs and cannot have or choose not to have a DIEP flap is the lateral thigh perforator (LTP) flap. Also called the “saddlebag” flap. The skin, fat, and other tissue is removed from the area in the upper outer thigh and upper buttock and moved to the chest. No muscle is taken.
Fat grafting is usually used for breast revisions or “touch up” surgeries. Your own fat is used to help fix any shape abnormalities that may be seen after the initial breast reconstruction surgery is done. The fat is not removed with skin, muscle, or other tissues.
The fat is obtained by liposuction, cleaned and then prepared so it can be injected easily into the areas it is needed. This is an outpatient procedure and you can go home the same day. Often, more then one session of fat grafting is needed to correct some contour deformities. This procedure has been found to be safe as far as cancer recurrence in patients who have had mastectomies.